PLC Injury
A PLC injury refers to damage to the posterolateral corner (PLC) of the knee, which includes a complex set of structures that stabilize the knee against varus (inward) forces, external rotation, and posterior translation. PLC injuries often occur alongside ACL or PCL injuries and can result from trauma, sports injuries, or motor vehicle accidents.
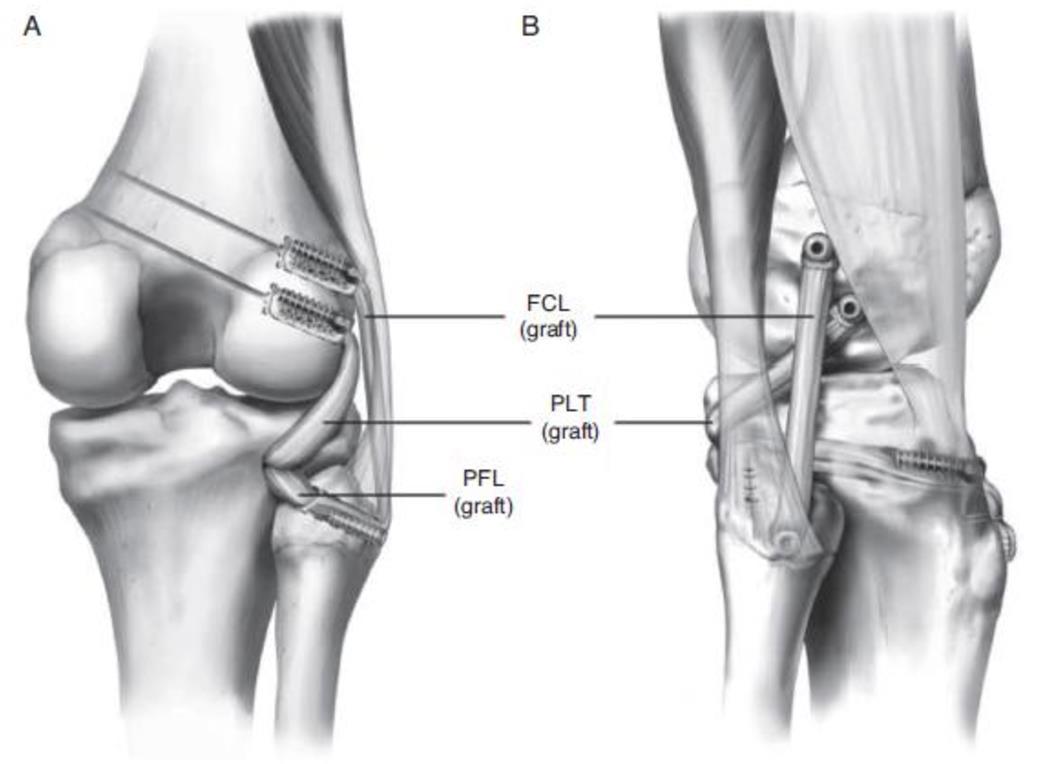
Anatomy of the PLC
The posterolateral corner consists of:
- Lateral collateral ligament (LCL) – Resists varus forces.
- Popliteus tendon – Assists in knee stabilization.
- Popliteofibular ligament – Prevents excessive external rotation.
- Other structures: IT band, lateral capsule, fabellofibular ligament.
Causes of PLC Injuries
- Direct trauma (e.g., a hit to the inner knee while the foot is planted).
- Hyperextension injury (e.g., falling awkwardly).
- Sports injuries (football, soccer, skiing).
- Motor vehicle accidents.
Symptoms
- Pain and swelling on the lateral (outer) side of the knee.
- Instability or giving way, especially when changing direction.
- Difficulty straightening the knee.
- Bruising or tenderness around the lateral knee.
- Nerve symptoms (if peroneal nerve is affected) – foot drop, numbness.
Diagnosis
- Physical tests: Varus stress test, dial test, external rotation recurvatum test.
- Imaging: MRI (best for soft tissue evaluation), X-rays (to check for fractures or dislocations).
Treatment Options
Non-Surgical
- For mild injuries (Grade I or II sprains):
- RICE (Rest, Ice, Compression, Elevation).
- Bracing and physical therapy to restore strength and stability.
- Anti-inflammatory medication.
Surgical
- For severe injuries (Grade III, complete tears, or instability):
- PLC reconstruction (using grafts).
- Repair of torn structures if possible.
- Combined surgery if ACL or PCL is also injured.
Rehabilitation & Recovery
- Non-surgical: 4-6 weeks of bracing and PT.
- Surgical: 6-12 months for full return to sports.
- Physical therapy focuses on restoring strength, range of motion, and proprioception.